|
|
||||||||||||||
|
IT SHOULD NOT HAPPEN TO YOU COMANCHE ACCIDENTS, 2.2003, AND A CASE by Omri Talmon Comanche Accidents, 2.2003 A particularly bad month: Seven accidents, including two fatal (five people). 2.1 Date: 02/02/2003 . Acft:: PA-24-250. DESCRIPTION: UPON LANDING ON RWY 13, PILOT ATTEMPTED TO COMPENSATE FOR WIND. THE NOSE STEERING DID NOT WORK, PILOT USED RIGHT BRAKE, LOSING CONTROL OF ACFT. ACFT SPUN OUT OF CONTROL OFF THE RUNWAY. UPON STOPPING THE MAIN LANDING GEARS COLLAPSED. One POB, no injuries. Damage: Minor. 2.2 Date: 02/05/2003. Acft: PA-24-180. DESCRIPTION: ON TAKEOFF, ACFT CAUGHT A TAILWIND THAT FORCED IT BACK DOWN. DAMAGE TO FRONT AND WING. Damage: Substantial. Two POB, both with minor injuries. 2.3 Date: 02/09/2003. Acft: PA-24-180. DESCRIPTION: ACFT LANDED GEAR UP. Damage: Minor. Two POB, no injuries. 2.4 Date: 02/06/2003. Acft: PA-24-250. DESCRIPTION: AIRCRAFT HAD TROUBLE MAINTAINING ALTITUDE AND HEADING. RADAR CONTACT WAS LOST AT APPROXIMATELY 2353Z ON 02/06/03. AIRCRAFT WRECKAGE WAS LOCATED ON 02/07/03 AT 1330Z APPROXIMATELY 6.2 MILES NW OF THE FLO VOR (FLORENCE, SC. Damage: Destroyed. Three POB, all fatally injured. 2.5 Date: 02/13/2003. Acft: PA-30. DESCRIPTION: LANDED RUNWAY 5 AND THE GEAR COLLAPSED. Damage: Minor. One POB, no injuries. 2.6 Date: 02/17/2003. Acft: PA-24-250. DESCRIPTION: ACFT LANDED GEAR UP. Damage: Minor. One POB, no injuries. 2.7 Date: 02/22/2003. Acft: PA-30. DESCRIPTION: ACFT CRASHED UNDER UNKNOWN CIRCUMSTANCES IN AN OPEN FIELD. Damage: Destroyed. Two POB, both fatally injured.
A CASE This time; A case from the United Kingdom. Please note the report is written in UK style for grammar and spelling.
Official Report
United Kingdom Bulletins (Dece
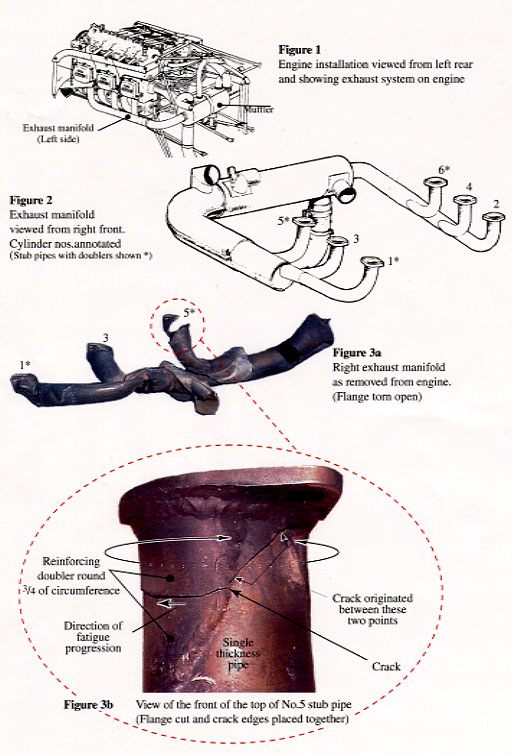
A Synopsis Whilst making a flight for the purpose of revalidating a Private Pilot's License (PPL), the pilot and instructor were both exposed to a dangerous level of carbon monoxide (CO) contamination from the engine exhaust gases. Their ability to fly the aircraft was impaired and the aircraft entered a spinning maneuver from which it did not recover. Both occupants died in the impact. It was established that exhaust gases had escaped from a fatigue crack, which had formed in one of the stub pipes close to its attachment flange at the cylinder head, and that the formation of this crack had been influenced by the presence of a reinforcing doubler welded to the pipe. The stub pipes, and the manifold of which they are an integral part, were manufactured in the USA by a company other than the aircraft manufacturer under a Part Manufacturing Authority (PMA) granted by the FAA, and obtained by the aircraft owners through a parts supply company. Although the aircraft manufacturer retains the Type Certificate for the aircraft, they no longer manufacture this part. The addition of reinforcing doublers, however, was not an acceptable change to the design in the opinion of the Type Certificate holder. No record of the installation of this manifold had been entered into the aircraft log books. History of flight The left seat pilot on the accident flight had been a part owner of G-ARIE since 1995. He had held a PPL since 1992 and his most recent revalidation for his single-pilot, single-engine rating had been 3 July 1999. He had a total of 265 hours flying experience of which 130 hours were on type. In accordance with Joint Aviation Requirements - Flight Crew Licensing (JAR-FCL) 1.245(c)(1), this revalidation was required every two years and, as a consequence, the pilot had made a private arrangement with a Qualified Flying Instructor (QFI) to fly a one hour dual flight in G-ARIE. No witnesses were found to confirm the intended profile of the flight although Aeronautical Information Circular (AIC) 127/1999 details the content of such a flight. The QFI had been a flying instructor since 1991. An acquaintance had sat with the two pilots before the flight and saw them walk out to G-ARIE. He saw the pilot sit in the front left seat and the QFI sit in the front right seat. One witness heard a sound of 'backfiring' during engine start but no other unusual events were reported. Takeoff appeared normal at approximately 1515 hrs. The acquaintance described the weather as 'CAVOK' with the surface wind as 10 to 12 kt from the northeast. Numerous eye witnesses, on the surface, near Osea Island saw the final maneuvers of G-ARIE. Most described it as being in a descent, pointing nose down and "spiraling" or "spinning". Additionally, a pilot who was flying a Yak 11 in the area also saw the aircraft spinning. This pilot was flying between 2,500 and 3,000 feet amsl when he saw the aircraft to his left and below him; he described it as being in a spin to the right with a nose down pitch attitude of about 60°. Initially, he thought that it was a training spin but became puzzled as it continued to spin and so he flew towards the area. He saw about four to six complete turns before the aircraft impacted the ground; as it did so, he saw a ring of spray from the crash site. Numerous personnel alerted the emergency services. The Yak pilot transmitted a 'Mayday' call on 121.5 Mhz and remained over the crash site until the emergency helicopters arrived; the 'Mayday' call was recorded at 1527 hrs. The RAF Search and Rescue (SAR) helicopter reported on the frequency at 1533 hrs and was in visual contact with the Yak at 1541 hrs. By 1547 hrs, the RAF helicopter, a police helicopter and an air ambulance helicopter were on the scene and had confirmed that the accident had been fatal. The police had recorded the first telephone call from the public at 1529 hrs. All the witnesses described the weather as very good with a clear horizon. The pilot of the RAF rescue helicopter estimated that the visibility was about 15 km although the horizon was "hazy". Eye witnesses Most eye witnesses only saw the aircraft when it was descending. Additionally, most confirmed that they were aware of aircraft in the area and that some of these aircraft had been doing aerobatics. Some witnesses commented on the fact that a jet aircraft was also flying in the area at low level. The Yak pilot stated that he did not see any other aircraft in the immediate area when he saw the spinning aircraft. Two independent witnesses stated that they saw the accident aircraft carrying out some maneuvers before entering a steep spiral descent. Some others considered that the aircraft had been flying straight and level before suddenly going into the descent. Most of the witnesses who saw the aircraft commented that there appeared to be little or no engine noise as it descended, and that there had been no fire or explosion when it struck the ground. Recordings A radio recording was available from 'London Area and Terminal Control Centre' on frequency 121.5 Mhz. This included the initial emergency call from the Yak pilot and the communication with the rescue helicopter, but there was no evidence of any emergency call from G-ARIE. A primary radar recording was obtained from National Air Traffic Services Ltd. This indicated that, after takeoff the aircraft initially maintained an easterly heading before taking up a north easterly heading. The initial primary radar contact was at 1514 hrs and the last contact was overhead Osea Island at 1527 hrs. The track was generally straight apart from two occasions when the aircraft turned through approximately 60° to the right for a short time before turning back to the left. Calculations from the radar recording indicated that the aircraft ground speed was approximately 120 kt for the first six minutes before reducing gradually to approximately 60 kt for a further four minutes. It then increased to approximately 140 kt over the next minute before reducing again to 60 kt before radar contact was lost. The radar recording did not show any indications of extreme maneuvering before the loss of contact. With no aircraft transponder operating, aircraft altitude could not be determined. Medical information Post-mortem examinations, including toxicology tests, were carried out on both pilots. Raised CO levels were found in both pilots, one of whom was a smoker but the carboxyhaemoglobin levels found were higher than would be seen in even the heaviest of smokers. The consensus of opinion from various specialists consulted by the pathologist, was that the levels were unlikely to be due to post mortem artifact and that they were indicative of CO inhalation during life. General Aviation Safety Sense Leaflet 24 on 'Pilot Health' includes a section on CO. This includes the comment that: 'The symptoms are subtle, similar to hypoxia but perhaps with a more obvious headache and it doesn't respond so promptly to oxygen - although using an oxygen mask is likely to restrict further exposure.' Aviation medical books include the important information that CO combines with hemoglobin some 200 times more easily than oxygen. These books also emphasize some physical symptoms of CO concentrations in the blood but have limited information on other aspects. Symptoms which are not well highlighted are confusion and impaired judgement. One publication stated it was important to note that the severity of symptoms did not correlate well with carboxyhaemoglobin levels. The CAA intend to reissue Leaflet 24 with additional information about CO and will reemphasize the dangers of CO in a future General Aviation Safety Information Leaflet (GASIL). Operational information The pilot had flown G-ARIE on 6 May 2001 for a one hour flight with a passenger who reported that there had been no problems with the aircraft and stated that neither of them had suffered any symptoms of CO poisoning. Following that flight, the pilot had refueled the aircraft with 88.09 litres of fuel; the normal procedure, used by the owners for the aircraft, was that it would be refueled to full after each flight. The aircraft did not fly again until the accident flight. The distance from Stapleford Airfield to Osea Island is 24 nm. At normal cruise airspeed of 150 kt and with a headwind component of 10 kt, this would have taken approximately 10 minutes. AIC 127/1999 details the content of the dual flight with a flight instructor. The flight should consist of four main sections: preflight and departure; general air work; emergency operations; arrival and landing. At the time of the accident, the pilots should have been involved with general air-work. This would involve the following aspects: climbing at best angle and best rate; straight and level cruising flight; steep turns - at not less than 45° of bank; recovery from the power off clean stall - fully developed; recovery from the approach to the stall in the landing configuration; recovery from the stall in the landing configuration whilst in the turn; recovery from the incipient spin. The Piper PA 24-250 Comanche is not cleared for aerobatics or intentional spinning. Stall speed with flap down is approximately 56 kt; stall speed clean is approximately 60 kt. The Piper Comanche Owner's handbook states that all the flight controls are effective down to the stalling speed and that stalls are gentle and easily controlled. Post accident calculations indicated that the aircraft was within normal C of G and weight limits. Crash site investigation Examination of the accident site showed that the aircraft had struck the ground in a very steep nose down attitude, estimated to be 70/75° to the horizontal. There had been no significant transitional movement of the aircraft after the initial impact, consistent with an essentially vertical descent, and the relative lack of fragmentation of the wreckage indicated a relatively low vertical speed of, probably, between 60 and 80 kt. There was a clear impression of where the wing leading edges had struck the ground, the imprint of the right wing being slightly lighter and curved whilst that of the left, was straight and heavier. The overall assessment indicated that the aircraft had struck the ground, steeply nose down, whilst spinning to the right. The three blades of the variable pitch propeller had folded straight backwards and exhibited only slight signs of circumferential scuffing. This, and the characteristics of the fractures of the propeller hub, caused by the blade roots being levered out, indicated that the propeller had been rotating at impact but with very little power applied. Examination of the wreckage at the accident site indicated that no significant components had separated from the aircraft before it struck the ground. Initial appraisal indicated that the landing gear had been retracted but it was not possible to determine the flap position. There was no clear evidence to indicate the position of any of the flying controls at impact. The aircraft's fuel tanks had been disrupted by the impact and were found to contain no fuel. There was, however, fuel present in the engine compartment fuel lines and evidence on the ground of a large fuel burst on both sides of the aircraft and from both ahead of and behind the wings. This indicated that there had been a considerable quantity of fuel in the tanks at the time of impact. Subsequent engineering investigation The wreckage was recovered to the AAIB facility at Farnborough for further examination. This confirmed that no components had separated from the aircraft before impact, that all the primary and secondary flying controls were correctly fitted and that there was no evidence of any controls having been restricted or jammed prior to the accident. The elevator trim mechanism was found to be set about 11/2 units nose up from the normal cruise position. The landing gear was confirmed to have been in the retracted position and the fuel selector was set to allow fuel to be drawn from both main wing tanks. Examination of the carburetor barrel, at the butterfly location, indicated that the throttle had most probably been at, or near to, fully closed at the time of impact. Examination of the flap lever ratchet mechanism revealed evidence which suggested that, at impact, it had been set at the first stage flap position. As a result of the raised CO level found in both pilots, particular attention was paid to the condition of the engine exhaust system and its attachment to the cylinder heads. Exhaust manifold description
Exhaust gasses from each cylinder flow into curved stub pipes which are attached to the cylinder head exhaust ports by a flange welded to the end of each pipe. Two threaded studs, which pass through the flange, a gasket and two nuts effect a gas tight joint. The three pipes from each side of the engine join together to form a stack (manifold), and the two manifolds connect with a muffler (silencer) located across the lower rear section of the engine. Two heater muffs are incorporated into this exhaust system, one around the silencer for cabin air, the other around the right manifold for carburetor hot air. The exhaust system is designated as an airframe component. Exhaust manifold examination Whilst the exhaust manifolds were being removed from the cylinder heads it was observed that all the attachment nuts appeared to have been tight before impact and that there was no evidence of significant exhaust blow-by on any of the flange faces. After they had been removed from the engine it was possible to observe that the cylinder head cooling fins, just forward and inboard of the No 5 cylinder head exhaust port, exhibited evidence of being affected by heat to a greater extent than those on the aft side of this port, or anywhere around the exhaust ports of the other cylinders. It was also observed that the exhaust manifold stub pipes from cylinders 1, 5 & 6 had reinforcing doubler plates welded over the basic stub pipes immediately below their attachment flanges, covering about two inches of pipe length and three quarters of their circumference, Figure 3b. After the manifolds had been removed, it was found that the attachment flange of the No 5 manifold stub pipe had been fractured at a point just aft of the forward inboard stud hole. From this location, another fracture ran in the wall of the stub pipe. As a result of impact forces, the flange and pipe had become severely twisted, Figure 3a, but the edges of the fractures of both the flange and the stub pipe wall showed no localized distortion. This indicated that both elements had been cracked right through prior to the impact. Subsequent metallurgical examination showed that the fractures in the stub pipe wall and doubler, and effectively all of the flange fracture, were due to fatigue, but the brightest portions of the pipe and doubler fractures, at their extremities, were areas of tearing overload. It was possible to distinguish, by inference, that the fatigue crack had originated at some point in the single thickness section of pipe between the flange and the doubler edge welds, Figure 3b. The oxidation and contamination of the crack surface by gas wash, however, precluded the determination of both the crack origin and how long it had existed. It was observed that the fracture in the doubler had propagated much faster than that in the basic pipe, and that the rate of propagation in both stub pipe and doubler had accelerated rapidly over the last few stress cycles, towards the point where the tearing overload had started. Examination of the other stub pipes of both manifolds revealed no evidence of any other fatigue cracking. Comparison of the heat discoloration on the No 5 pipe with that on the other stub pipes showed that it did not, after the accident, exhibit any significantly different marking or discoloration, particularly along the line of the fracture. Any discoloration might have been of assistance in identification of the crack's existence before the accident. The cabin air heat exchanger and carburetor heat muff were both dismantled and the normally obscured parts of the exhaust system examined for evidence of exhaust gas escape, but none was found. Maintenance The aircraft had a valid Certificate of Air worthiness in the Private Category and had been maintained, by members of the owning group, in accordance with the CAA Light Aircraft Maintenance Schedule (LAMS/A/1999). For an aircraft in this Category a licensed pilot, who is the owner or operator, may perform a 50 hour/6 monthly check, or any of the other maintenance tasks prescribed in Air Navigation (General) Regulation 16, and act as the signatory in the appropriate log book. All other maintenance and inspection tasks are required to be certificated by an appropriately approved maintenance organization or Licensed Engineer, although the maintenance tasks themselves may be done by unlicensed personnel. The most recent inspection of the aircraft had been a 50 hr/6 month check, performed by a member of the owning group. This had been the first inspection since the most recent Annual Inspection, which had been carried out by an Approved Maintenance Organization in June 2000. In both of these inspections, examination of the exhaust system was specifically identified as a requirement. Compliance with Air worthiness Directives on both the manifolds and the muffler was mandatory at the Annual Inspection. There was nothing, in either the current aircraft log books (from January 1989 onwards) or any of the documentation received from the Approved Maintenance Organization, to indicate that the exhaust manifolds had been repaired or changed at any time. The owners stated, however, that the manifolds had been changed relatively recently but were able to produce only an invoice, dated 22 January 1999 and relating to a right hand manifold, as documentary support. On this invoice the manifold Part No is given as 23537-002 RB, which is not listed in the aircraft Parts Catalogue, nor is it a Part No applied to any design of manifold approved by the Type Certificate holder. Presuming that this Invoice was related to the approximate date of fitting of this part, it indicated that the manifold had been fitted to the aircraft at some time between the previous Annual Inspection, in December 1998, and the subsequent 50 hour check. If this is correct, the manifold had been fitted for about 150 flying hours. The manifold in question had not been obtained from the aircraft manufacturer, who no longer makes this part, but from an independent supplier in the USA. It is understood that this supplier obtains them, in turn, from another company with a PMA granted to them by the FAA. The invoice document included a statement certifying that the part supplied had been 'manufactured and inspected in accordance with the air worthiness regulations of the United States'. This implied that the part had been made in accordance with a design drawing approved by the FAA and that it should have been accompanied by the necessary certificate of compliance. The design of the exhaust manifolds, which were previously produced by the aircraft manufacturer, who both retains the 'Type Certificate' and remains the design authority for this aircraft type, did not have reinforcing doublers below the manifold attachment flanges. Their opinion was that such a feature would not be considered acceptable either as a concession at construction or for a subsequent repair, as it would, probably, give rise to localized and unpredictable thermal stress cycles. Previous carbon monoxide poisoning events The CAA provided information, from Mandatory Occurrence Reporting data relating to suspected CO poisoning, that since July 1996 there have been a total of eight cases involving piston engined aircraft. Of these, seven had CO detectors fitted and in each case the detector indicated the presence of CO; defects likely to have resulted in CO leakage into the cabin were subsequently identified in six of these aircraft. During the course of this investigation, information was also received from the owner/pilot of a similar Comanche aircraft whose aircraft had a CO sensor, of the 'spot' type, stuck on the instrument panel. Just before takeoff, he observed that the 'spot' had turned black, indicating the presence of CO. As a result he abandoned the intended flight and, before making a subsequent short flight for a thorough maintenance inspection of the exhaust system, obtained an electronic CO meter which complied with BS 7860:1996. After engine start for the flight to the maintenance organization, the pilot observed indicated CO concentrations in the cockpit of up to 45 ppm during the ground preparation and run-up checks. The levels observed during the subsequent flight were very low. The pilot obtained information on this equipment through an Avweb internet site using the search criteria 'carbon monoxide + aircraft'. This also yields many other sites with contents related to this subject. Discussion a) Probable cause of the accident The two pilots seemed in normal spirits prior to the flight. The start and takeoff appeared uneventful, apart from one witness report of "backfiring" during engine start. Once airborne, the radar indications were that the aircraft maintained a relatively straight track, apart from two deviations, directly towards the area of Osea Island. The next reports from eye witnesses were of an aircraft spinning continuously until it hit the ground; there was some confliction in the reports as to whether the aircraft was maneuvering prior to this spin. The ground marks at the accident site were indicative of an aircraft spinning, with little engine power at the time of impact. Subsequent post mortem examination of the pilots indicated that they had inhaled CO during life. Following this finding, the investigation concentrated on the flight profile for evidence of incapacitation and on the aircraft systems for evidence of a CO leak. The radar recording had no indication of altitude but ground speed could be calculated. This indicated a variation in speed from close to normal cruising speed, a reduction to about stall speed, an increase to cruise speed and a second reduction to about stall speed until radar contact was lost. One possibility for this variation would be if the pilots were carrying out stalls as detailed in the dual check AIC. However, prior to stalls, normal airmanship would be for the pilots to carry out 'clearing turns' prior to any maneuvering; although two track diversions were noted, these were not as comprehensive as would normally be expected. A more likely possibility would be that the pilots were incapacitated to the extent that they made no, or a minimal, input to the controls during this 'cruise'. In that case, the speed variation could have occurred in sympathy with a cyclic variation in aircraft altitude. However, the aircraft eventually departed from level flight into a spinning maneuver. To spin, an aircraft needs to be stalled and to be subjected to a yaw. The stall could have occurred during the cyclic variation and any yaw input could have been made by one of the pilots while he was under the influence of CO poisoning and confused by events. However, during the investigation, it was established from radar recordings that G-ARIE went out of control at a position in which another aircraft had been some 55 seconds before. If G-ARIE had encountered some wake turbulence from this other aircraft, it could have resulted in an upset and subsequent loss of control. It was not possible to establish the precise chain of events but with some of the known effects of CO poisoning, inappropriate inputs to the flight and engine controls by one or both of the pilots was a distinct possibility. Regardless of the final chain of events, both the pilots were suffering from CO poisoning after a short time in flight and the engineering examination of the wreckage revealed that there had been a preexisting fracture in the No 5 stub pipe of the right exhaust manifold. This would have resulted in exhaust gases (including CO) being discharged into the engine compartment/nose landing gear bay space and, from there, these would have passed, through any less than perfect seal on the bulkhead and nose-gear bay, to the cockpit. (The experience of the other Comanche owner would indicate that exhaust gas ingress to the cockpit can be high between engine start and takeoff and this may have been a significant factor in this accident). Since the human respiratory system has a much greater tendency to absorb CO than Oxygen, very little leakage through the bulkhead seals would be required to create a dangerously high concentration of CO in the cabin atmosphere. An overview of the results of medical research conducted over a long period has indicated that the levels of carboxyhaemoglobin found in both crew members was consistent with their having breathed an atmosphere with a 0.1% CO concentration for about 20-30 minutes. Behavioral tests have indicated that the level of carboxyhaemoglobin found in both occupants would have been likely to affect their judgement seriously and incline them to take inappropriate actions. b) Stub pipe failure mechanism It was not possible to determine whether the exhaust discoloration of the fins on the No 5 cylinder head had been the result of a long exposure to a slight leak, a short exposure to a large leak, or something between these conditions. The surviving passenger from the previous occasion that G-ARIE had been flown stated that neither she or the pilot had suffered any ill effects from that flight. It is more probable, therefore, that the fracture in the exhaust pipe became critical at engine start, or early in the accident flight, and resulted in a very large increase in the rate of leakage of exhaust gas. This would be consistent with the apparently unusually rapid onset of the effects of CO inhalation on the aircraft's occupants. The failed manifold was obtained from an Approved source in the USA and, although a certifying statement on the sales invoice appeared to indicate that it was an approved part, FAA Form 8130-3, Air worthiness Approval Tag, has not been produced. The manifold did not conform precisely to the design of the aircraft manufacturer, who is still the holder of the Type Certificate, and the changes made were considered likely to induce unpredictable stress cycles in the locality of the reinforcing doublers. The metallurgical examination of the No 5 stub pipe established that the fatigue crack had initiated somewhere between the two welds which bordered the single thickness portion of the pipe in which the spiral part of the fracture ran, Figure 3. The spiral nature of the fracture over this portion indicated the presence of some torsional stress in this zone, in a clockwise sense looking down on the flange. Apart from this loading, the welding on of reinforcing doublers was likely to have introduced an unpredictable mixture of localized stresses into the pipe, amongst which would likely be some residual torsional stress. The presence of these doublers, which were not in intimate contact with the basic pipe except at the welds, would also have given rise to very different thermal, and consequently stress, cycles in the pipe and doubler. These stresses would result from the different rates at which the pipe and doubler would be likely to heat and cool during power changes, particularly at engine startup. The additional local stiffness induced by the presence of the doublers would also have affected the stress cycles. Any of these stresses would be likely to have been more critical in the single thickness part of the pipe, over the length where the doublers existed, but unpredictably so owing to the complexity of the combination of temperature distribution, thermal expansion and residual stress effects in that zone. It seems probable that a combination of these effects and the local stiffening of the zone, by the presence of the doublers keeping the fracture tightly closed, may also have allowed the fracture to develop to a critical length before it became practically possible to detect it by visual inspection. c) Maintenance Procedures The general philosophy used to determine appropriate inspection frequencies for the detection of cracks is that it should be possible for a crack to remain undetected at one inspection interval and not become critical before the next. The inspection interval required by the manufacturer for the exhaust system is stated to be 100 flying hours, but this is over-ridden by the requirement in LAMS that it should be inspected every 50 hrs. Although the importance of examining the manifold and the gasket seals is clearly stated in all information on exhaust inspection, the emphasis tends to be more focussed on the danger from possible defects in the cabin air heat exchanger. Another issue, recognized and the subject of part of Air worthiness Notice No 40, is the integrity of the sealing of the firewall bulkhead between the engine compartment and the cabin. This is where a number of apertures, which allow the passage of controls or services, have seals which may deteriorate with age or use. The maintenance records for this aircraft indicated that all the requisite inspections, including those of the exhaust system, had been completed correctly since the time that the owners stated that the exhaust manifold had been changed. Although the required record of fitting of this manifold was not made in the aircraft log books, the examination of the manifolds did not reveal any evidence to suggest that they had been wrongly fitted or that there had been any difficulty with their installation. After installation, it would only have been possible to inspect the area of the exhaust manifold in which the crack occurred using a mirror and light. The post crash inspection of the No 5 stub pipe did not reveal any evidence of local discoloration on the pipe outer surface, which might have assisted in revealing the crack during inspection. The lack of such discoloration also suggested that the crack had not opened up significantly prior to this flight. It is also uncertain that the discoloration of the cylinder head around the manifold attachments, which was seen after removal of the manifold from the engine, would have been readily noticed during this kind of inspection. Certification of the Manifold The manifold which contained the crack was not constructed in accordance with the design of the Type Certificate holder. The modified design, to which the manifold was constructed by the company with the PMA, should have been approved by the FAA as being as good as, or superior to, the design of the Type Certificate holder. The wording on the invoice, certifying that the manifold had been 'manufactured and inspected in accordance with the airworthiness regulations of the United States', implies that the Supplier of the manifold to the aircraft owners was of the belief that such approval had been granted. However, the absence of any other documentation associated with the fitting of this new manifold has prevented attempts to establish if the part fitted had been properly manufactured and approved. Carbon monoxide detectors The ingress of CO was clearly not apparent to either pilot during the accident flight, and the lack of a CO detector may have been a factor. Records indicate that over the last five years, there have been eight reported instances of pilot's becoming aware of CO ingress because of the change in colour of the detector. There is no current requirement to fit detectors in aircraft although aviation publications highlight the possibility of and risks associated with CO poisoning. General Aviation Safety Sense Leaflets 3B (Winter Flying) and 24 (Pilot Health) refer to the dangers of CO poisoning and the availability of 'spot' type of detectors. Both publications emphasize that the detectors have a limited life and need to be changed frequently. Additionally, General Aviation Safety Information Leaflet 1 of 2001 included an article on CO poisoning based on an incident reported in AAIB Bulletin 12/2000. Although they have a limited effective life and are vulnerable to the fumes of some cleaning fluids, the spot type of CO detectors are cheap and readily available. It would seem sensible, therefore, for all piston engine powered aircraft to carry one in a position clearly visible to the pilot. Although it would not be expected that spot type detectors could offer total protection, when considering the insidious nature of the onset of symptoms, and the potentially lethal effects of CO inhalation, the carriage of such a detector is likely to improve the chances of early detection of the presence of this gas. Electronic detectors, which are capable of quantifying the level of CO contamination in the atmosphere, and which are made to meet a British Standard, are also available. Safety recommendations With regard to the foregoing, the following safety recommendations are made: Safety recommendation 2002-23 The Civil Aviation Authority should develop an appropriate recognized performance specification against which carbon monoxide detectors can be assessed and approved, with the eventual aim of mandating their use on all piston engined aircraft. Safety Recommendation 2002-30 In the absence of it being mandatory for all piston engined aircraft to carry a carbon monoxide detector, the Civil Aviation Authority should vigorously promote that all such aircraft should have a current carbon monoxide detector fitted to facilitate an early warning of the presence of this gas. Safety recommendation 2002-24 The Federal Aviation Administration should review the acceptability of the design of the exhaust manifold for the Piper PA-24-250, as produced by organizations other than the type Certificate Holder and, together with the Parts Manufacturing Authority holders, take action as necessary to prevent further occurrences of manifold cracking. Published 12 December 2002 MY DISCUSSION This report is long, detailed, and seemingly very comprehensive. However, I dare say that there is a noticeable emphasis on the regulatory aspect (whether the exhaust pipe was or was not approved) while other issues relevant to the case are not discussed. Exhaust pipes, whether approved or not, can and do crack. Is it a reason for CO to penetrate the cockpit? It should not be. In this case, with only 13 minutes elapsed since takeoff (maybe more time for taxi) both pilots inhaled CO in an alarming amount. There must have been a very serious firewall breach that was not mentioned in the report. An example: The rubber nose wheel steering rod boots are torn, even missing, or otherwise not keeping the firewall air tight. Could it be that several other feedthrough openings were not properly sealed? Even so, one wonders how such a massive CO penetration could occur. Is it possible that the heater was on and it had a leak as well, so in lieu of ventilating the cockpit with warm air it further aggravated the situation? Another possibility is that the outlet of the cabin air duct was not properly connected, or was blocked. Another source of exhaust gas ingress (particularly in slow flight) is through the wing root area (the rubber molding strips are supposed to stop this) and inspection panels in the floor. However, this, too, is unlikely to generate sufficient quantities in such a short time. The report does not address these issues. As to the exhaust pipe, folks familiar with the systems of the 250 advise that they have seen factory fitted exhausts with these doublers and they are a very common feature. Yes, they can crack, but no more so than a single flange pipe. One just has to look more carefully for cracks. The facts in this accident are that both pilots had CO poisoning, and the aircraft spun into the ground with the engine at a low ("little") power level, from a speed of about 60 Kt. The pilots (the instructor with zero time in type, the owner with relatively low time), with their judgment and actions impaired by CO, may have been trying a stall. It deteriorated into a spin from which they did not manage to recover. CO related accidents are very rare. Nevertheless, and quite typically, the AAIB makes recommendations to regulate and mandate CO detectors. This should be left to the pilots. I personally flew for many years with a "spot type" detector and now, together with quite a few who are known as "the Choir", have switched to an electronic device which is part of the flying bag, not the aircraft. Finally, one should keep in mind that twins can also have elevated CO levels in the cockpit due to heater problems.
Lessons Pay good attention to the exhaust stacks whenever possible. There should be proper muffler support brackets fitted (exhaust hangers in the twin). The firewall should be a fire wall, not a kitchen grate.
Proverb For every action, there is an equal and opposite government program.
Omri Talmon, born in 1936, lives in Tel Aviv, Israel. He holds degrees in engineering, business administration and accounting. Presently a consultant, he worked for many years as an executive for several hi-tech companies. Omri is a private pilot with both Israeli and U.S. certificates. His ratings include SEL, MEL, Instrument, Glider, and CFI (glider). Since 1974 he owns and flies a 1966 PA-30-B, registration 4X-CAO.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||